The best illicit way to improve performance in an endurance sport like road cycling is blood doping. This concept encompasses a series of techniques and/or substances that have a common goal: to increase the mass of red blood cells, which in turn will allow better oxygen transport to the muscle and thus a noticeable increase in performance. Two techniques can be highlighted as the most used: on the one hand, autologous blood transfusions, and on the other, injections of recombinant human erythropoietin (rHuEPO). Fortunately (and unfortunately for the cheater), antidoping testing (and its sensitivity) has improved markedly, which combined with the 4-year sanctions “awarded” for these misdemeanors has made the athlete tempted to illegality think twice or resort to alternative methods. In the next paragraphs, I will review in a little more detail the two most notorious blood doping methods as well as the alternatives that the 2022 cheater may be resorting to.
Blood transfusions
In the past and until the introduction of the biological passport, it was possible to resort to transfusions of important blood volumes (450-1000ml) with little fear of being caught and with performance benefits that could exceed 10% in a highly trained athlete (which, in elite sport, is an enormous difference in performance). With the ADAMS system, biological passport and 4-year sanctions, this type of transfusion has become a thing of the past in elite cycling. However, microtransfusions, with their lesser impact on the biological passport, and their more than appreciable effect on performance (more than 5% in trained athletes after reinfusion of 130ml of homologous blood) may constitute a viable, potentially safe and quite attractive alternative for the cheater.
rHuEpo
The theoretical basis for the use of rHuEpo in performance enhancement is clear and is supported by numerous studies in trained athletes showing improvements of up to 10% in maximal oxygen uptake after a regular cycle of this substance. However, conventional doses (just like a regular blood transfusion) are relatively easy to catch as ATPF (Atypical Biological Passport Finding). Although this may not lead to an immediate sanction, it will serve to initiate strategic tests that will sooner or later bring the cyclist to an antidoping court. The same cannot be said for microdoses of rHuEPO, which, according to the available evidence, can improve performance of a trained athlete by more than 4% (as Andersen demonstrated in an excellent paper this year) and are much more difficult to be detected with the current testing methods.
Current anti-doping issues
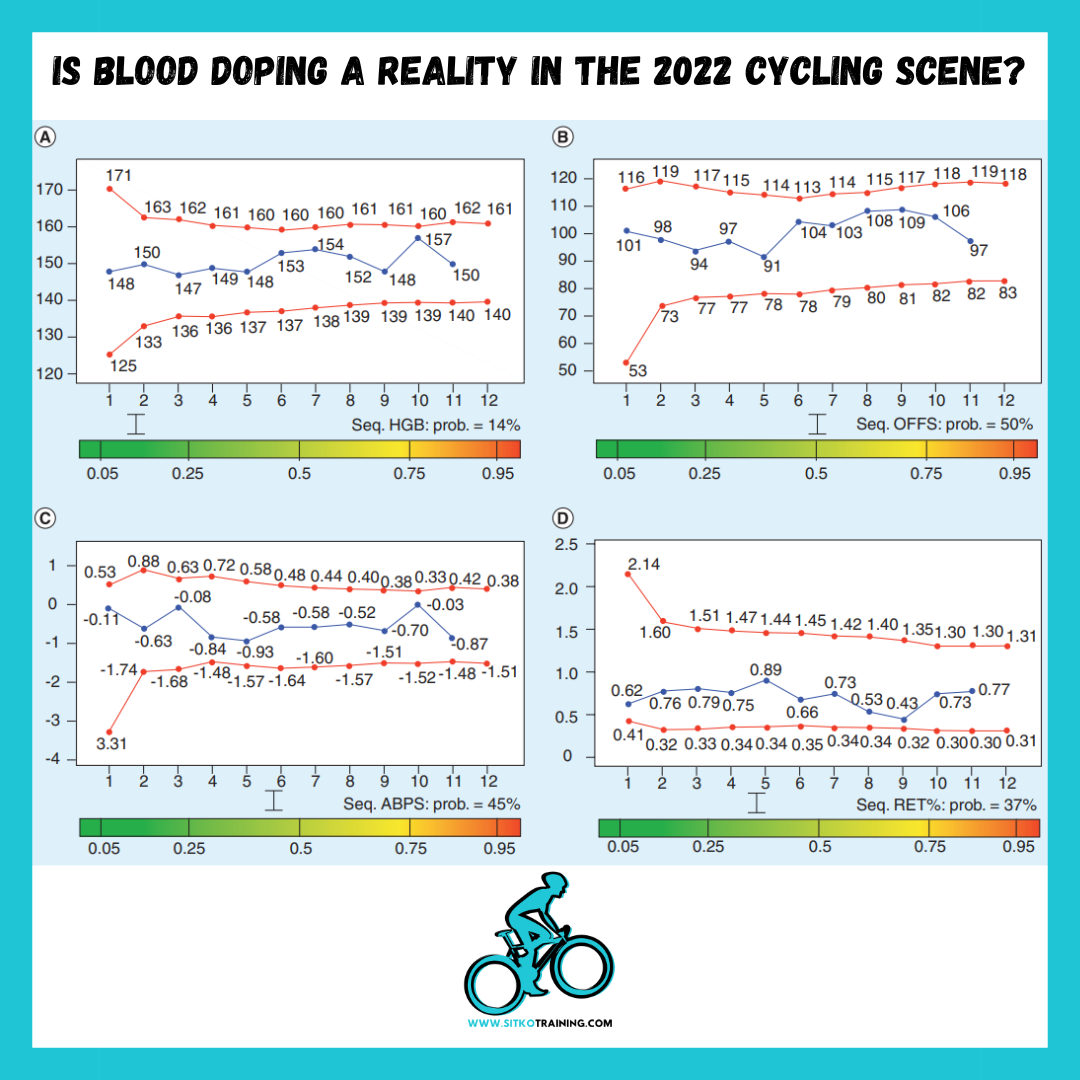
The ADAMS system linked to the biological passport has marked a turning point in the fight against blood doping. Despite this, the system has clear shortcomings that can be perfectly exploited by the cheater. The biological passport includes the monitoring of 12 hematological parameters derived from a scale based on the percentage of reticulocytes and hemoglobin (OFF-Hr) and another multifactorial scale (ABPS). The application of personal thresholds in these scales (by means of Bayesian statistics) makes it possible to find “non-standard findings” in 45-100% of cases of conventional blood doping, an amount that varies depending on the literature. Therefore, and this must be made very clear to the reader, the biological passport DOES NOT DETECT all cases of conventional blood doping, but only a fraction of them, a fact that reinforces what I have believed since its implementation: its main purpose is dissuasive.
The problem appears when we assess the reliability of the same system in the cases of microdosing: the detection capacity is reduced to 20-60% depending on the literature. The immediate future is promising in this regard, with new biomarkers such as the fraction of immature reticulocytes or the ratio of immature reticulocytes/red cells. These biomarkers will make it possible to increase the capacity to detect cases of doping with microdoses of rHuEPO and, to a lesser extent, small blood reinfusions. However, the thresholds for these biomarkers have not yet been scientifically established and, therefore, a major question mark remains regarding their use. In addition, and this deserves further comment, in order to initiate a disciplinary procedure, an abnormal finding in the biological passport must be unanimously verified by three experts, also taking into account various factors such as the altitude at which the sample was taken, the competition schedule, the explanation provided by the athlete, etc. In short, this process is far more complex than pointing out an “outlier” in a graph and imposing a 4-year sanction on the cheater.
Does blood doping exist in the current road cycling scene?
It’s a complicated question because any answer can be compromising. I do believe that blood doping exists today but it is extremely residual, and not because of a lack of willingness. I am not naive and in this aspect I am a faithful follower of Hobbes: what really moves man is his fear and his selfishness. With the measures established in the last decade, we have tipped the balance of risk/benefit in favor of those of us who desire a clean sport: those who want to dope with a transfusion or rHuEPO know that they have a certain possibility of being caught, which added to the 4 years of potential sanction and, let’s not forget, retrospective testing, make doping a very unprofitable practice today. Could some cyclists/doctors/teams be escaping from the control of the system? Yes, without a doubt, especially by resorting to the already commented microdoses. But I honestly don’t think that the performance increase we’ve seen in the World Tour in recent years is due to a widespread return to blood doping, as I’ve seen suggested on social media from time to time.
I honestly believe this is an exceptional generation of riders who train better than ever, eat better than ever, rest better than ever, and I won’t say they use gear that is better than ever because of my well-known disc brake phobia. There are some black sheep, sure, but I am very skeptical about the possibility that blood doping could be substantially altering the results of the highest category of cycling in the middle of the year 2022. Indeed, we have made some progress although there is still a lot of work to be done: Given our shortcomings at the detection level, we must increase the dissuasive purpose of anti-doping testing. 1) Lifetime sanctions should already be a reality for blood doping/anabolic steroid use, as I have always defended. 2) Economic penalties should be increased for anti-doping rule violations and 3) Staff with a past related to doping should be removed from the World Tour (and there are quite a few that should be removed). With these measures in place my confidence in a totally clean top level cycling would increase exponentially, but we are still far from that point.
Sebastian Sitko
Professor at the University of Zaragoza, PhD in Sports Sciences, Master in High Performance Sports by the French Olympic Committee, National Cycling, Athletics and Triathlon Coach and official coach for the American College of Sports Medicine.
Recommended papers:
Andersen, A. B., Graae, J., Bejder, J., Bonne, T. C., Seier, S., Debertin, M., … & Nordsborg, N. B. (2022). Micro-doses of Recombinant Human Erythropoietin Enhance Time Trial Performance in Trained Males and Females. Medicine and Science in Sports and Exercise.
Ashenden, M., Gough, C. E., Garnham, A., Gore, C. J., & Sharpe, K. (2011). Current markers of the Athlete Blood Passport do not flag microdose EPO doping. European journal of applied physiology, 111(9), 2307-2314.
Bejder, J., Aachmann‐Andersen, N. J., Bonne, T. C., Olsen, N. V., & Nordsborg, N. B. (2016). Detection of erythropoietin misuse by the Athlete Biological Passport combined with reticulocyte percentage. Drug Testing and Analysis, 8(10), 1049-1055.
Bejder, J., Solheim, S. A., Gybel-Brask, M., Secher, N. H., Johansson, P. I., & Nordsborg, N. B. (2019). Time Trial Performance Is Sensitive to Low-Volume Autologous Blood Transfusion. Medicine and science in sports and exercise, 51(4), 692-700.
Durussel, J., Daskalaki, E., Anderson, M., Chatterji, T., Wondimu, D. H., Padmanabhan, N., … & Pitsiladis, Y. P. (2013). Haemoglobin mass and running time trial performance after recombinant human erythropoietin administration in trained men. PloS one, 8(2), e56151.
Haile, D. W., Durussel, J., Mekonen, W., Ongaro, N., Anjila, E., Mooses, M., … & Pitsiladis, Y. P. (2019). Effects of EPO on blood parameters and running performance in Kenyan athletes. Medicine and science in sports and exercise, 51(2), 299-307.
Heuberger, J. A., Rotmans, J. I., Gal, P., Stuurman, F. E., van’t Westende, J., Post, T. E., … & Cohen, A. F. (2017). Effects of erythropoietin on cycling performance of well trained cyclists: a double-blind, randomised, placebo-controlled trial. The Lancet Haematology, 4(8), e374-e386.
Pottgiesser, T., Sottas, P. E., Echteler, T., Robinson, N., Umhau, M., & Schumacher, Y. O. (2011). Detection of autologous blood doping with adaptively evaluated biomarkers of doping: a longitudinal blinded study. Transfusion, 51(8), 1707-1715.
Solheim, S. A., Bejder, J., Breenfeldt Andersen, A., Mørkeberg, J., & Nordsborg, N. B. (2019). Autologous blood transfusion enhances exercise performance—strength of the evidence and physiological mechanisms. Sports medicine-open, 5(1), 1-11.